Neurology & Psychiatry · 2015
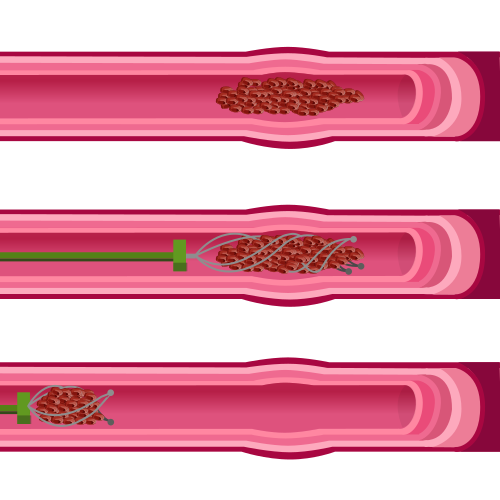
Endovascular thrombectomy trials (MR CLEAN and HERMES)
MR CLEAN: Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands; HERMES: Highly Effective Reperfusion evaluated in Multiple Endovascular Stroke trials
Through the first decade of the 2000s, every well-designed trial of intra-arterial stroke therapy had failed. IMS III, MR RESCUE, and SYNTHESIS were all stopped or reported negative results between 2012 and 2013, and the common conclusion was that catheter-based clot removal simply did not improve outcomes beyond intravenous tPA. Stroke neurologists and interventionalists continued to debate whether the problem was patient selection, imaging criteria, procedure timing, or device technology. The answer turned out to be all four at once.
MR CLEAN, published in the New England Journal of Medicine in January 2015, was the first randomized controlled trial to show a definitive benefit. Diederik Dippel and colleagues at Erasmus University Medical Center in Rotterdam enrolled 500 patients with angiographically confirmed proximal large-vessel occlusion at 16 Dutch centers and randomized them to mechanical thrombectomy plus usual care or usual care alone. Functional independence at 90 days, defined as a modified Rankin Scale score of 0 to 2, was achieved by 32.6% of the intervention group versus 19.1% in the control group. No ceiling on time from onset was imposed, though most patients were treated within 6 hours.
Four concurrent trials, ESCAPE, EXTEND-IA, SWIFT PRIME, and THRACE, were all halted early after their data safety monitoring boards reviewed the MR CLEAN data. Those trials had stricter imaging selection criteria, faster door-to-groin times, and exclusively used second-generation stent retrievers, the Solitaire and Trevo devices, which had substantially higher recanalization rates than the older Merci coil retriever used in the earlier failed trials. The 2016 HERMES meta-analysis, led by Mayank Goyal at the University of Calgary and Jeffrey Saver at UCLA, pooled 1,287 patients across all five trials. The absolute benefit translated to one additional independent survivor for roughly every 2.6 patients treated, an effect size unusually large for an acute intervention.
The speed of adoption was without recent precedent in stroke medicine. Within months of the MR CLEAN publication, centers across North America and Europe restructured protocols to provide around-the-clock interventional coverage. Stroke systems of care shifted toward regionalization, with spoke hospitals bypassing closer facilities to route large-vessel occlusion patients directly to thrombectomy-capable centers. The window for treatment later extended to 24 hours in selected patients based on the DAWN and DEFUSE 3 trials, which used perfusion imaging to identify salvageable penumbra.
What the MR CLEAN result demonstrated was as much methodological as clinical. Earlier trials had not required confirmed proximal occlusion on vascular imaging before randomization, meaning large proportions of enrolled patients had no retrievable clot. Better imaging selection, not better devices alone, explained much of the reversal from the failed trials of 2012 and 2013.
Key People
- Diederik Dippel — Principal investigator of MR CLEAN
- Mayank Goyal — Led the HERMES collaborative meta-analysis
- Jeffrey Saver — Co-lead of HERMES; calculated number-needed-to-treat
- Olvert Berkhemer — First author of the MR CLEAN trial publication
- Tudor Jovin — Contributed to the HERMES pooled analysis; later led the DAWN trial
N Engl J Med. 2015 (MR CLEAN); Lancet. 2016 (HERMES)
Related landmarks
- 2018 · DAWN: extended-window thrombectomy (Neurology & Psychiatry)
- 2019 · Esketamine (Spravato) for treatment-resistant depression (Neurology & Psychiatry)
- 2023 · Lecanemab (CLARITY AD): anti-amyloid antibody for Alzheimer disease (Neurology & Psychiatry)
- 2006 · STAR*D sequenced antidepressant treatment study (Neurology & Psychiatry)