Critical & Organ Care · 1937
First clinical use of heparin as an injectable anticoagulant
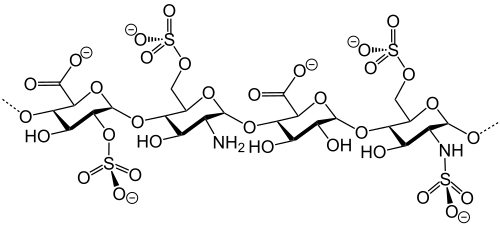
Anticoagulation in the 1930s was theoretically possible but practically limited. Heparin had been discovered at Johns Hopkins in 1916 by Jay McLean, then a medical student, who isolated a phospholipid fraction with anticoagulant properties while working in William Howell's laboratory. The compound attracted interest but resisted clinical application for two decades because the extracts available were too impure and too toxic to inject into patients safely. Researchers attempting heparin in animals routinely encountered febrile reactions, hemolysis, and hypotension that were attributable to contaminating substances rather than to heparin itself.
The purification problem was solved at the University of Toronto. Charles Best, already known for his role in the insulin work of 1921, directed a team that developed a standardized, purified heparin preparation from beef liver and later from beef lung. The key steps involved removing pyrogens and ensuring consistent potency, expressed in standardized units. Gordon Murray, a surgeon at Toronto General Hospital, used this preparation in clinical patients beginning in 1937, first for peripheral venous thrombosis and then for more complex vascular problems. Murray, along with L. B. Jaques, T. S. Perrett, and Best, published their results in Surgery that year.
Access to a reliable, rapidly reversible parenteral anticoagulant extended into nearly every technical domain of surgery and critical care. By the mid-1950s, heparin was an essential component of the heart-lung bypass circuit that John Gibbon and others were developing for open cardiac surgery. Hemodialysis required anticoagulation of the extracorporeal circuit; heparin provided it. Vascular surgery, arterial catheterization, and cardiopulmonary bypass all depended on the ability to anticoagulate predictably and to reverse anticoagulation with protamine when needed.
Heparin's mechanism was clarified over subsequent decades. It binds antithrombin III and accelerates its inhibition of thrombin and factor Xa by orders of magnitude. The requirement for antithrombin III meant that patients with hereditary deficiency were heparin-resistant, a clinical observation that retrospectively explained some early failures. Low-molecular-weight heparins, developed in the 1970s and reaching clinical use in the 1980s, offered improved subcutaneous bioavailability and more predictable pharmacokinetics by acting preferentially on factor Xa rather than thrombin.
Unfractionated heparin remains in use today for situations where rapid onset, short half-life, and reversibility with protamine are required, including cardiopulmonary bypass, acute coronary syndromes, and bridging during procedures. Its continued presence in clinical practice alongside newer anticoagulants reflects properties that direct oral agents do not replicate: immediate reversal, activity in the extracorporeal circuit, and decades of dosing experience in high-acuity settings.
Key People
- Gordon Murray — Toronto surgeon who performed the first clinical heparin injections
- Charles Best — Physiologist whose lab produced the purified, standardized heparin preparation
- Jay McLean — Johns Hopkins medical student who first isolated anticoagulant heparin in 1916
- L. B. Jaques — Co-author of the 1937 Surgery paper; contributed to purification and standardization work
Norman R. CMAJ. 2011 (free history review of the 1937 first clinical use)
Related landmarks
- 1943 · Kolff's rotating drum artificial kidney (Critical & Organ Care)
- 1916 · Rous and Turner's citrate-glucose method for storing red blood cells (Critical & Organ Care)
- 1960 · Scribner shunt and long-term hemodialysis (Critical & Organ Care)
- 1968 · Harvard Criteria for Brain Death (Critical & Organ Care)