Critical & Organ Care · 2013
PROSEVA prone positioning in severe ARDS
Proning Severe ARDS Patients
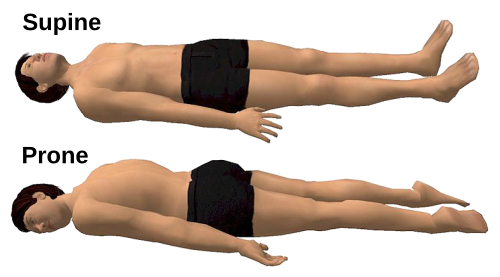
The physiological rationale for prone positioning in ARDS has been understood since the 1970s. In the supine position, the dependent posterior lung regions bear the weight of edematous tissue and receive a disproportionate share of ventilation, while the dorsal regions remain partially collapsed. Rotating a patient prone redistributes perfusion and opens dorsal alveoli, reducing ventilation-perfusion mismatch and cyclical collapse. What was missing for decades was a trial that could demonstrate whether this physiological improvement translated to a survival benefit.
Several randomized trials in the 2000s tested prone positioning without finding a mortality reduction. Those earlier studies enrolled heterogeneous ARDS populations, used proning sessions of eight hours or fewer, and included sites with varying levels of experience in the technique. Claude Guerin at Croix-Rousse Hospital in Lyon identified two factors he believed explained the null results: insufficient session duration and insufficient restriction to the most severely hypoxemic patients.
PROSEVA, which Guerin led, randomized 466 patients with severe ARDS at 26 ICUs in France and one in Spain. Eligibility required a PaO2 to FiO2 ratio below 150 on standardized ventilator settings within 36 hours of intubation. The prone group received sessions of at least 16 consecutive hours per day. Twenty-eight-day mortality was 16.0% in the prone group versus 32.8% in the supine group; at 90 days the figures were 23.6% and 41.0%, respectively. The independent data monitoring committee stopped the trial at the second planned interim analysis. Jean-Marie Reignier contributed to enrollment and data collection across the participating centers.
The result was striking in magnitude, but the trial also illustrated why context matters in procedural interventions. The participating units had substantial experience with proning, and the protocol required careful attention to endotracheal tube security, hemodynamic monitoring during turns, and prevention of pressure injuries. Implementing the protocol outside experienced centers risked replicating the intervention without replicating the expertise. This tension between trial results and real-world implementation became a recurring theme when COVID-19 arrived.
During the COVID-19 pandemic, PROSEVA became the principal evidence base for prone positioning in mechanically ventilated patients with COVID-19-associated ARDS, and prone positioning rates in ICUs increased substantially. The protocol was also extended informally to awake, non-intubated patients on supplemental oxygen, a practice the PROSEVA trial did not evaluate and for which evidence from subsequent trials was inconsistent. The 16-hour minimum session duration and the severe ARDS threshold from PROSEVA remain the standard benchmarks in current intensive care society guidelines.
Key People
- Claude Guerin — Principal investigator; designed and led the PROSEVA trial at Croix-Rousse Hospital.
- Jean-Marie Reignier — Co-investigator; contributed to patient enrollment and data management.
- Luciano Gattinoni — Described physiological basis of prone positioning in ARDS; informed PROSEVA design.
N Engl J Med. 2013;368:2159-2168.
Related landmarks
- 2001 · Rivers Early Goal-Directed Therapy for Sepsis (Critical & Organ Care)
- 2000 · ARDSNet ARMA low tidal volume ventilation trial (Critical & Organ Care)
- 1989 · First Successful Living-Donor Liver Transplant (Critical & Organ Care)
- 1980 · Exogenous surfactant therapy for neonatal respiratory distress syndrome (Fujiwara) (Critical & Organ Care)