Surgery & Anesthesia · 2000
FDA Clearance of the da Vinci Surgical System
Laparoscopic surgery had been expanding since the late 1980s, driven by the benefits of smaller incisions, less postoperative pain, and faster recovery. The limitation was ergonomic and technical: instruments moved in counterintuitive directions through fixed ports, the two-dimensional camera reduced depth perception, and fine motor tasks in tight anatomical spaces strained even experienced surgeons. These constraints had held back adoption in procedures requiring precise suturing or complex dissection near critical structures. Robotic assistance was proposed as a way to restore the dexterity and visualization of open surgery while keeping the access advantages of a minimally invasive approach.
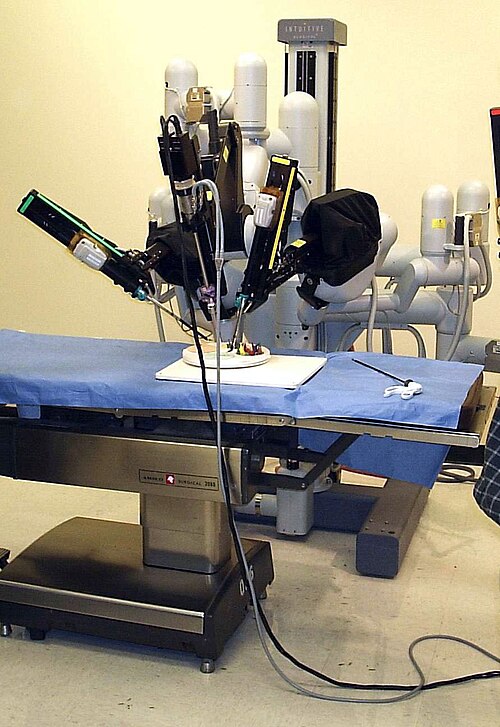
In July 2000 the FDA cleared Intuitive Surgical's da Vinci Surgical System under 510(k) premarket notification K990144 for general laparoscopic procedures. The system used three or four robotic arms controlled from a seated console, a three-dimensional high-definition endoscopic camera, and wristed instruments that replicated seven degrees of freedom and filtered out hand tremor. The surgeon sat at the console in a non-sterile field while the patient-side cart and a surgical assistant managed the operative field. Frederic Moll, a co-founder of Intuitive Surgical, had led the commercial development that brought the platform through FDA review.
Early adoption was slow. The capital cost of the system was substantial, running to roughly one million dollars per installation, and training requirements were considerable. Hospitals that acquired the system needed to recoup that investment through procedural volume, which created institutional pressure to expand indications. Radical prostatectomy became the primary application after early comparative series reported lower estimated blood loss and shorter hospital stays compared with open retropubic prostatectomy. Mani Menon at Henry Ford Hospital in Detroit developed a systematic technique for robotic prostatectomy and trained surgeons widely, which accelerated diffusion of the procedure.
By the early 2010s, robotic radical prostatectomy accounted for the majority of prostatectomies performed in the United States. The system extended into hysterectomy, colectomy, and cardiac procedures over the same period. High-quality randomized comparisons, however, consistently showed outcomes that were similar to standard laparoscopy or open surgery across most applications, with the exception of metrics like blood loss and transfusion rates where robotic prostatectomy held a reproducible advantage. The gap between adoption rates and comparative efficacy data became a recurring theme in surgical outcomes research and raised questions about how new surgical technologies should be evaluated before widespread adoption.
Intuitive Surgical's monopoly on the cleared robotic surgery market lasted nearly two decades before competitors entered the field. The FDA subsequently cleared several competing systems beginning in the late 2010s. Questions about complication reporting, device-related adverse events, and the learning curve for individual surgeons drew regulatory and journalistic scrutiny during that period, and the da Vinci system became the central example in ongoing debates about postmarket surveillance of surgical devices.
Key People
- Frederic Moll — Co-founder of Intuitive Surgical; drove the da Vinci system to market
- Mani Menon — Pioneered the robotic radical prostatectomy technique at Henry Ford Hospital
- Alvin Goh — Early adopter and trainer in robotic urologic surgery technique
U.S. FDA 510(k) K990144, Intuitive Surgical da Vinci Surgical System. 2000.
Related landmarks
- 2009 · WHO Surgical Safety Checklist (Surgery & Anesthesia)
- 1985 · First Laparoscopic Cholecystectomy (Surgery & Anesthesia)
- 1983 · Pulse oximetry enters routine clinical monitoring (Surgery & Anesthesia)
- 2021 · Genetically Modified Pig-to-Human Kidney Xenotransplant (Surgery & Anesthesia)